“Muscle recruitment and coordination with an ankle exoskeleton.” Journal of Biomechanics")
Journal article in Journal of Biomechanics:
How do muscle activations and synergies change when an individual wears an ankle exoskeleton during gait?
Abstract: Exoskeletons have the potential to assist and augment human performance. Understanding how users adapt their movement and neuromuscular control in response to external assistance is important to inform the design of these devices. The aim of this research was to evaluate changes in muscle recruitment and coordination for ten unimpaired individuals walking with an ankle exoskeleton. We evaluated changes in the activity of individual muscles, cocontraction levels, and synergistic patterns of muscle coordination with increasing exoskeleton work and torque. Participants were able to selectively reduce activity of the ankle plantarflexors with increasing exoskeleton assistance. Increasing exoskeleton net work resulted in greater reductions in muscle activity than increasing exoskeleton torque. Patterns of muscle coordination were not restricted or constrained to synergistic patterns observed during unassisted walking. While three synergies could describe nearly 95% of the variance in electromyography data during unassisted walking, these same synergies could describe only 85–90% of the variance in muscle activity while walking with the exoskeleton. Synergies calculated with the exoskeleton demonstrated greater changes in synergy weights with increasing exoskeleton work versus greater changes in synergy activations with increasing exoskeleton torque. These results support the theory that unimpaired individuals do not exclusively use central pattern generators or other low-level building blocks to coordinate muscle activity, especially when learning a new task or adapting to external assistance, and demonstrate the potential for using exoskeletons to modulate muscle recruitment and coordination patterns for rehabilitation or performance.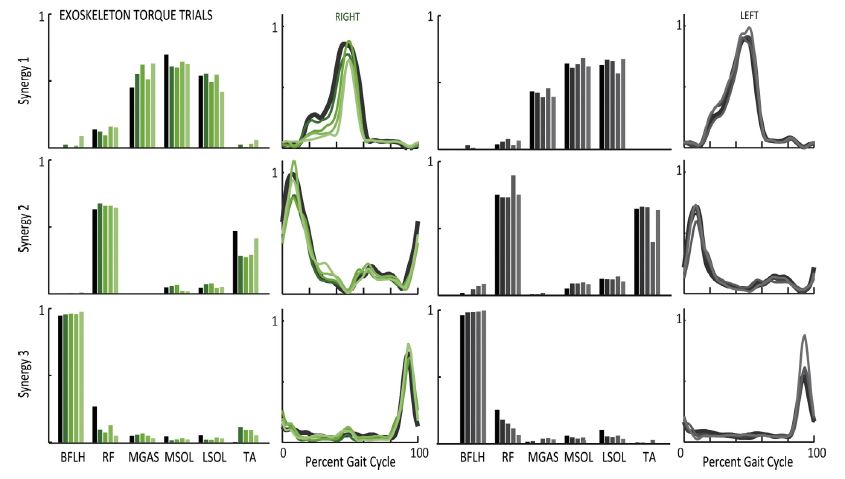

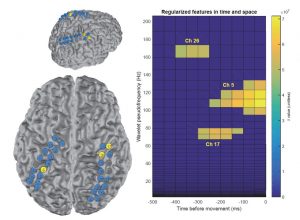
 “Multistep model for predicting upper-limb 3D isometric force application from pre-movement electrocorticographic features.” IEEE Engineering Medicine & Biology")

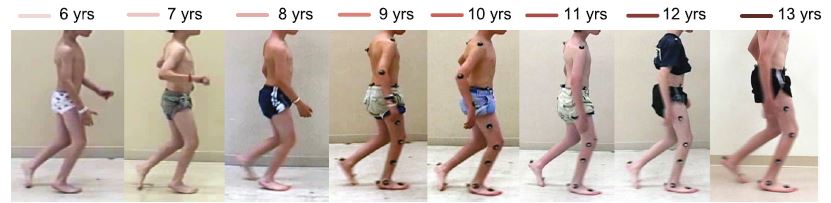
 “Clinical motion analyses over eight consecutive years in a child with crouch gait: a case report.” Journal of Medical Case Reports")