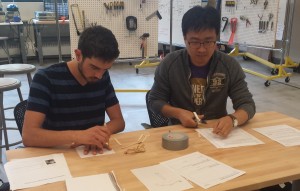
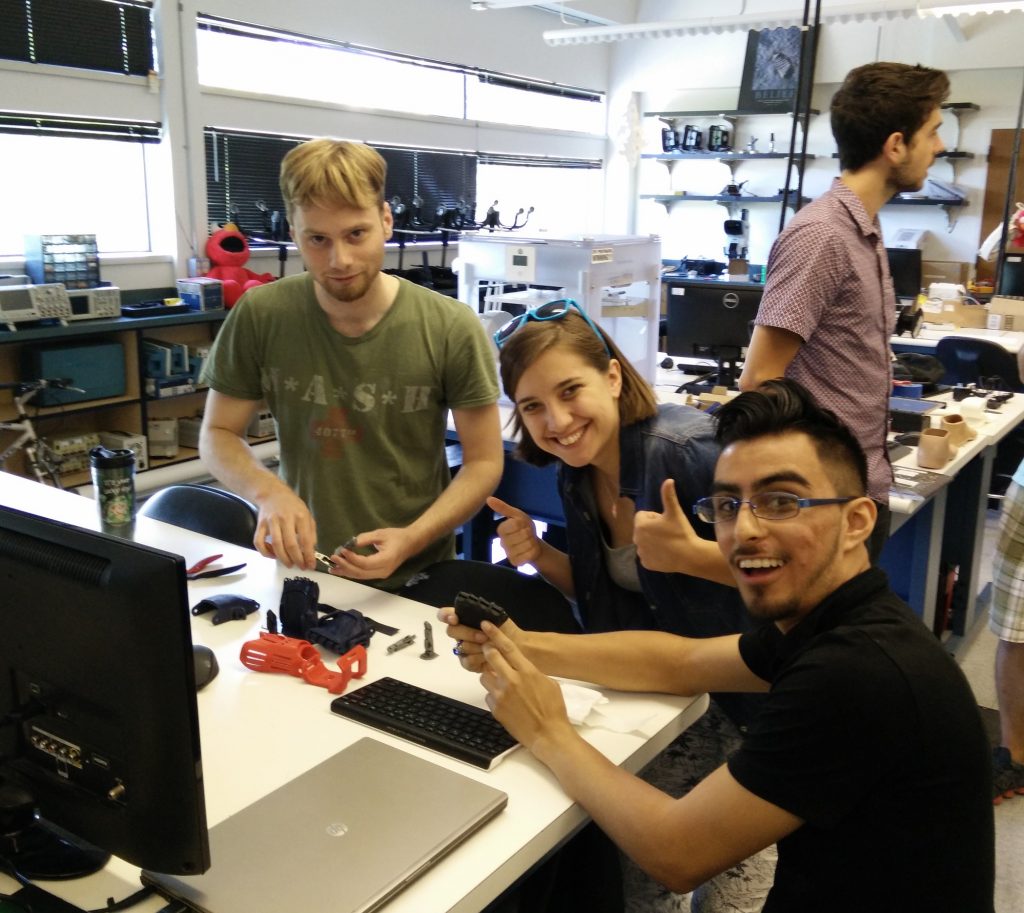
Today we hosted a prototyping challenge at the CoMotion Makerspace with some of our partners from Seattle Pacific University. The focus of today’s challenge was to both introduce our new lab members to low-resolution prototyping and improve the design of our affordable hand exoskeleton for individuals with impaired hand function.

The challenge:
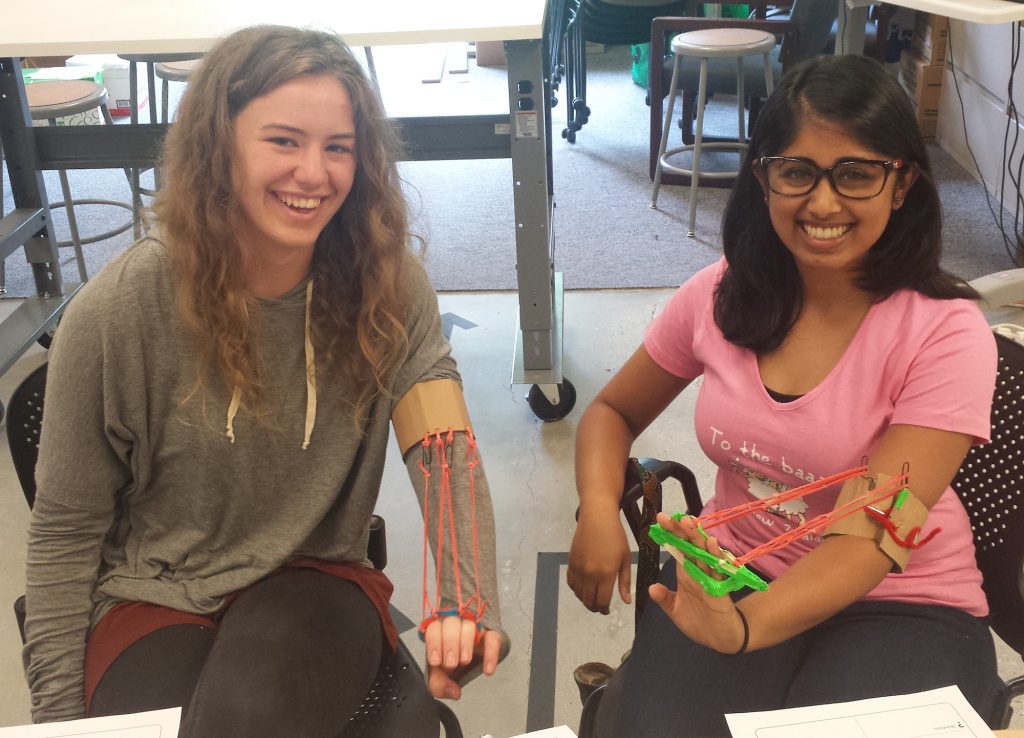
Individuals who have had a stroke or neurologic injury commonly lose the ability to open their hand. Physical and occupational therapy are the most common treatments and can lead to improvements in hand function with prolonged, focused practice. Exoskeletons and other robotic technology has been introduced, but these systems are typically expensive, bulky, and can only be used in the clinical environment. In this prototyping challenge, you will build and test low-resolution prototypes to explore how we might safely, comfortable, and affordably help to open the hand for individuals with neurologic disorders.
The group came up with some great ideas and designs (and some spectacular failures with important lessons). If you would like to try this prototyping challenge yourself, grab some prototyping supplies and work through our GUIDE.