Journal Article in Experimental Brain Research
Individuals with cerebral palsy (CP) display motor control patterns that suggest decreased supraspinal input, but it remains unknown if they are able to modulate lower-limb reflexes in response to more complex tasks, or whether global motor control patterns relate to reflex modulation capacity in this population.
 Aim: To further elucidate the multifaceted effects of CP on inhibitory and faciliatory supraspinal pathways and global measures of motor control, providing novel information for improving targeted neuromuscular interventions in this patient population.
Aim: To further elucidate the multifaceted effects of CP on inhibitory and faciliatory supraspinal pathways and global measures of motor control, providing novel information for improving targeted neuromuscular interventions in this patient population.
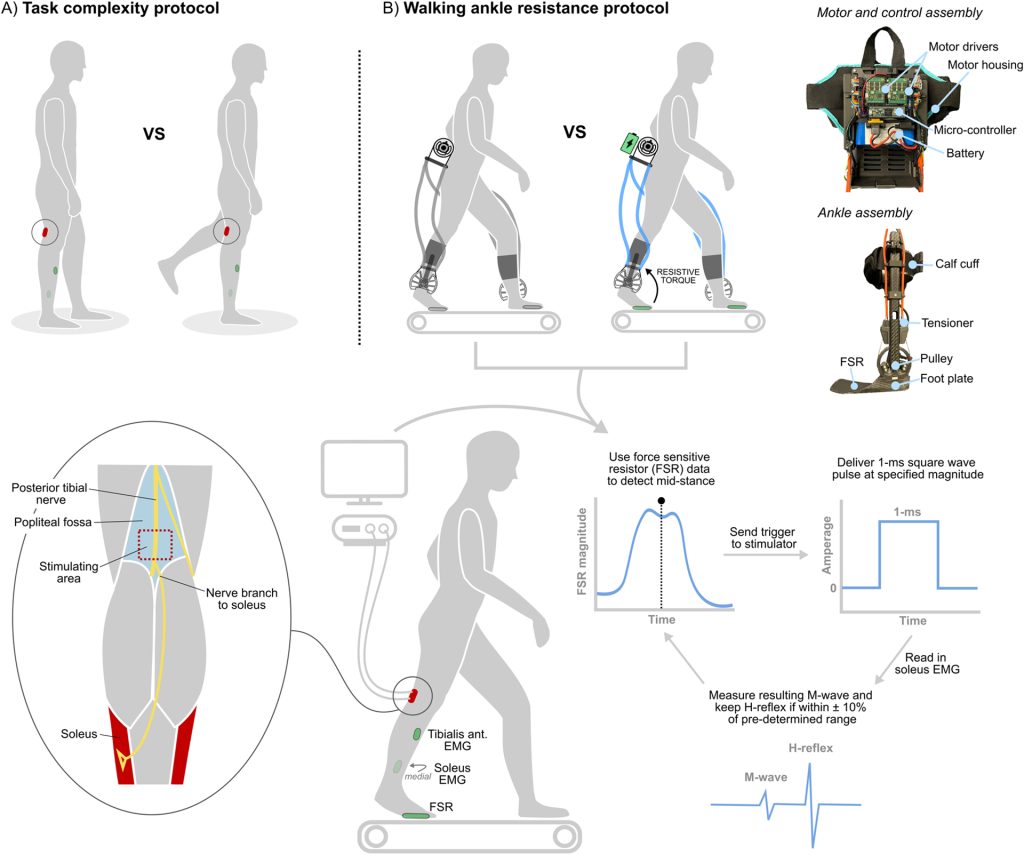
Methods: Eight ambulatory individuals with CP (12–18 years old) were recruited to complete a task complexity protocol, where soleus H-reflex excitability was compared between bilateral (baseline) and unilateral (complex) standing. We also investigated the relationship between each participant’s ability to modulate soleus H-reflex excitability and the complexity of their walking neural control pattern determined from muscle synergy analysis. Finally, six of the eight participants completed an exoskeleton walking protocol, where soleus H-reflexes were collected during the stance phase of walking with and without stance-phase plantar flexor resistance.
Results: Participants displayed a significant reduction in soleus H-reflex excitability (− 26 ± 25%, p = 0.04) with unilateral standing, and a strong positive relationship was observed between more refined neural control during walking and an increased ability to modulate reflex excitability (R = 0.79, p = 0.04). There was no difference in neuromuscular outcome measures with and without the ankle exoskeleton (p values all > 0.05), with variable reflex responses to walking with ankle exoskeleton resistance.
Interpretation: These findings provide evidence that ambulatory individuals with CP retain some capacity to modulate lower-limb reflexes in response to increased task complexity, and that less refined neural control during walking appears to be related to deficits in reflex modulation.