Journal article in Journal of Electromyography and Kinesiology:
In collaboration with Rehabilitation Medicine here at the University of Washington, we evaluated muscle use of 20 unimpaired participants during three upper-extremity functional tests. An interactive supplement can be found HERE.
 Background: Performance-based tests, such as the Jebsen Taylor Hand Function Test or Chedoke Arm and Hand Activity Inventory, are commonly used to assess functional performance after neurologic injury. However, the muscle activity required to execute these tasks is not well understood, even for unimpaired individuals. The purpose of this study was to evaluate unimpaired muscle recruitment and coordination of the dominant and non-dominant limbs during common clinical tests.
Background: Performance-based tests, such as the Jebsen Taylor Hand Function Test or Chedoke Arm and Hand Activity Inventory, are commonly used to assess functional performance after neurologic injury. However, the muscle activity required to execute these tasks is not well understood, even for unimpaired individuals. The purpose of this study was to evaluate unimpaired muscle recruitment and coordination of the dominant and non-dominant limbs during common clinical tests.
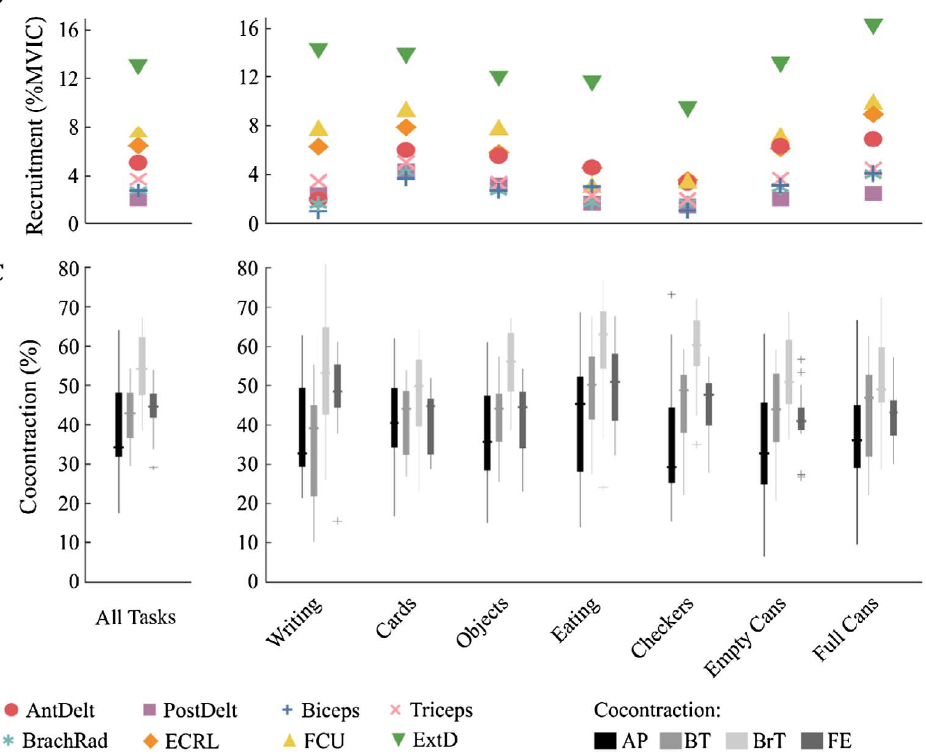
Methods: Electromyography (EMG) recordings from eight arm muscles were monitored bilaterally for twenty unimpaired participants while completing these tests. Average signal magnitudes, activation times, and cocontraction levels were calculated from the filtered EMG data, normalized by maximum voluntary isometric contractions (MVICs).
Results: Overall, performance of these functional tests required low levels of muscle activity, with average EMG magnitudes less than 6.5% MVIC for all tests and muscles, except the extensor digitorum, which had higher activations across all tasks (11.7 ± 2.7% MVIC, dominant arm). When averaged across participants, cocontraction was between 25 and 62% for all tests and muscle pairs.
Conclusion: Tasks evaluated by speed of completion, rather than functional quality of movement demonstrated higher levels of muscle recruitment. These results provide baseline measurements that can be used to evaluate muscle-specific deficits after neurologic injury and track recovery using common clinical tests.
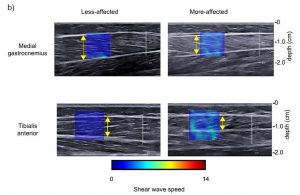
 Our skeletal muscles have amazing structure. They provide elegant and efficient actuation to move and explore our worlds. But how do we understand how muscles produce movement?
Our skeletal muscles have amazing structure. They provide elegant and efficient actuation to move and explore our worlds. But how do we understand how muscles produce movement? “Use of shear wave ultrasound elastography to quantify muscle properties in cerebral palsy.” Clinical Biomechanics")