Members of the lab attended the Neural Control of Movement (NCM) conference in Kobe, Japan, bringing together an international community focused on understanding how the brain controls movement.
Dr. Kat Steele presented at the satellite meeting on “Precision neurorehabilitation for movement disorders: Integrating technology, neuroscience, and clinical practice,” where she also organized a session on gait and mobility. Her talk, “On time mobility: Neuromechanics to support early play and participation,” highlighted the lab’s work at the intersection of biomechanics and neurorehabilitation.
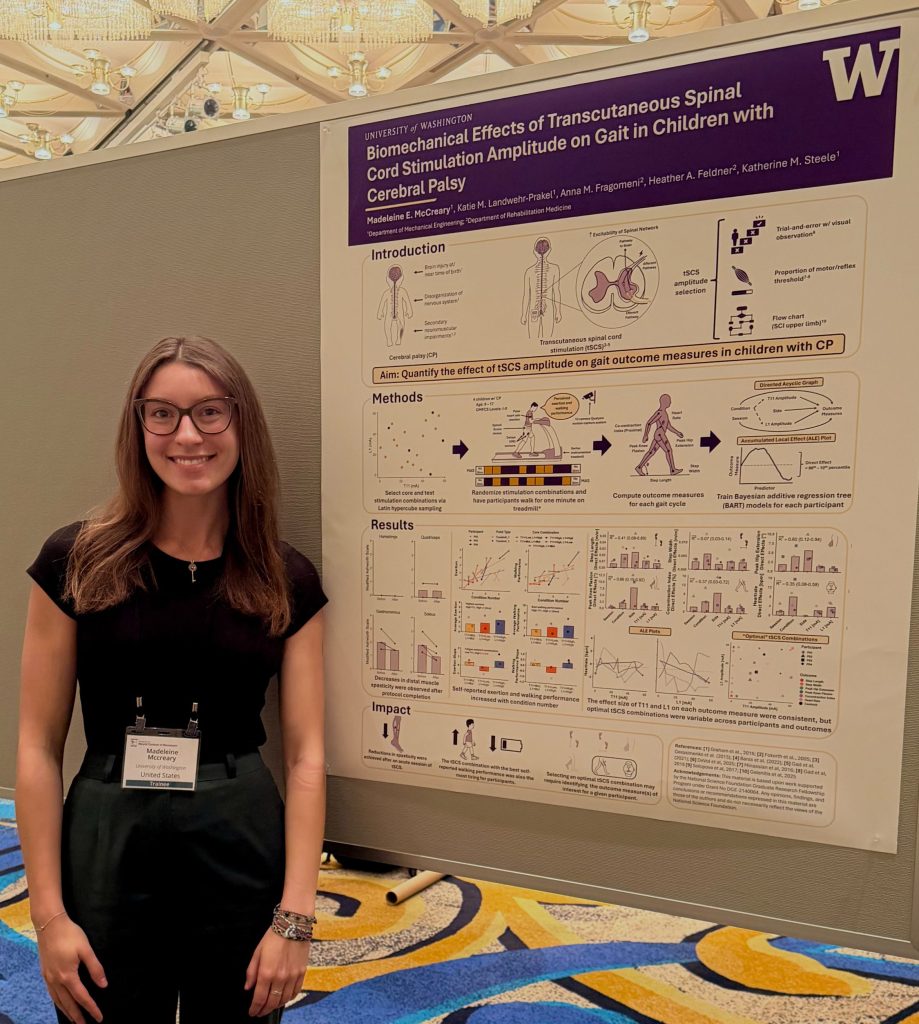
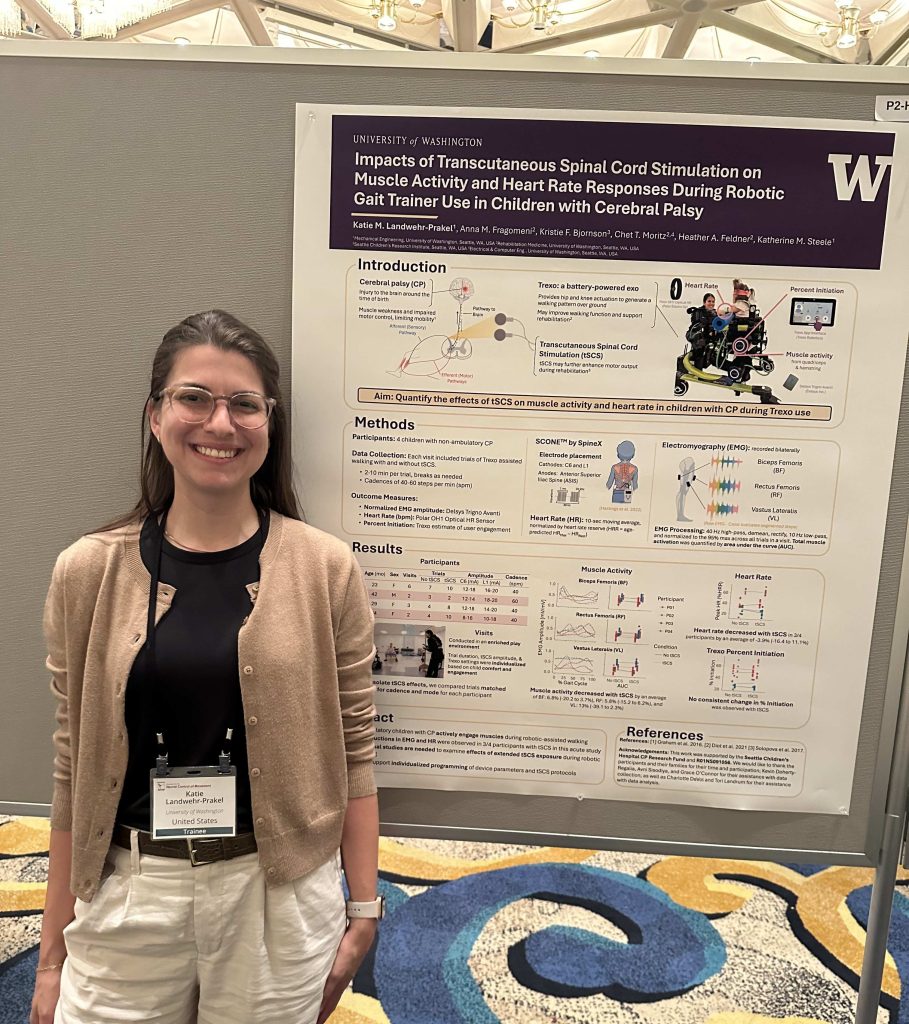
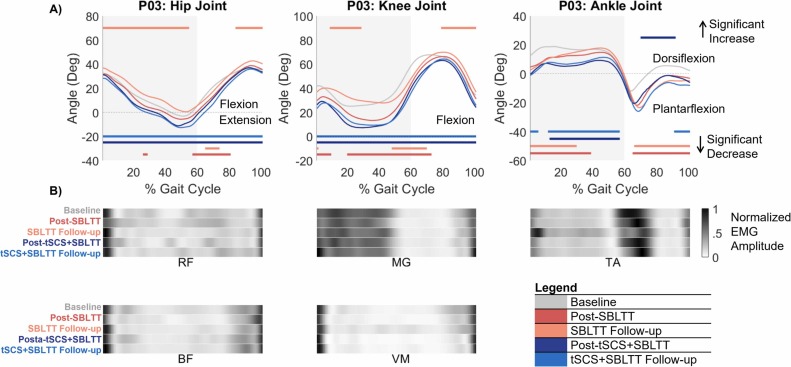
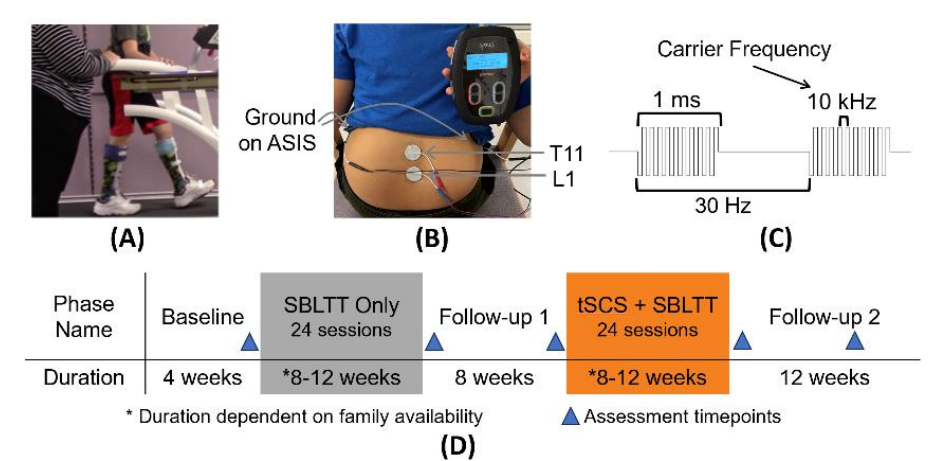
Madeleine McCreary presented a poster on “Biomechanical effects of transcutaneous spinal cord stimulation amplitude on gait in children with cerebral palsy.” And Katie Landwehr‑Prakel also presented a poster on “Impacts of transcutaneous spinal cord stimulation on muscle activity and heart rate responses during robotic gait trainer use in children with cerebral palsy.”
We were also excited to connect with lab alum and collaborator Dr. Charlotte DeVol, highlighting the strong ongoing collaborations within our broader research community.
It was an exciting opportunity to share research, connect with collaborators, and engage with the global NCM community.