Journal Article in Disability & Rehabilitation: Assistive Technology:
The accessibility of the built environment is an important factor to consider when providing a mobility device to a young child and their family to use in the community.
Aim: To quantify the driving patterns of children using an adapted ride-on car in their home and community environment over the course of a year using an integrated datalogger.
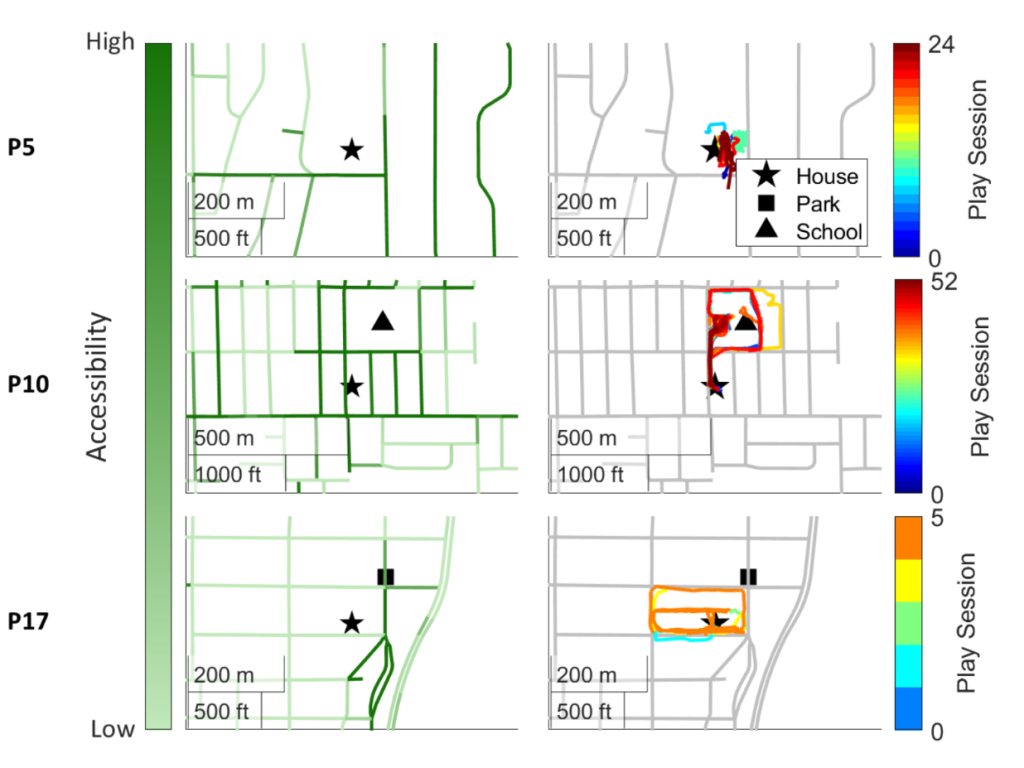
Method: Fourteen children (2.5 ± 1.45 years old, 8 male: 6 female) used adapted ride-on cars outside and inside of their homes over the course of a year. We tracked their device use metrics with a custom datalogger and geospatial data. To measure environmental accessibility, we used the AccessScore from Project Sidewalk, an open-source accessibility mapping initiative, and the Walk Score, a measure of neighborhood pedestrian-friendliness.
Results: More play sessions took place indoors, within the participants’ homes. However, when the adapted ride-on cars were used outside the home, children engaged in longer play sessions, actively drove for a larger portion of the session, and covered greater distances. Most children tended to drive their ROCs in close proximity to their homes. Most notably, we found that children drove more in pedestrian-friendly neighborhoods and when in proximity to accessible paths.
Interpretation: The accessibility of the built environment is paramount when providing any form of mobility device to a child. Providing an accessible place for a child to move, play, and explore is critical in helping a child and family adopt the mobility device into their daily life.