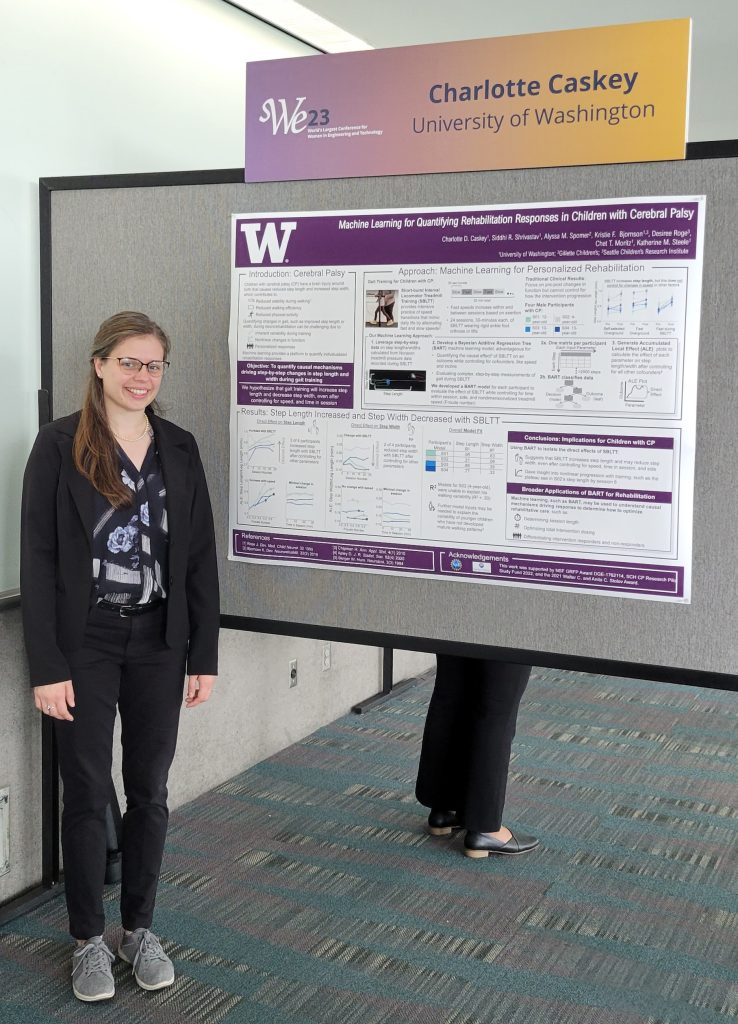
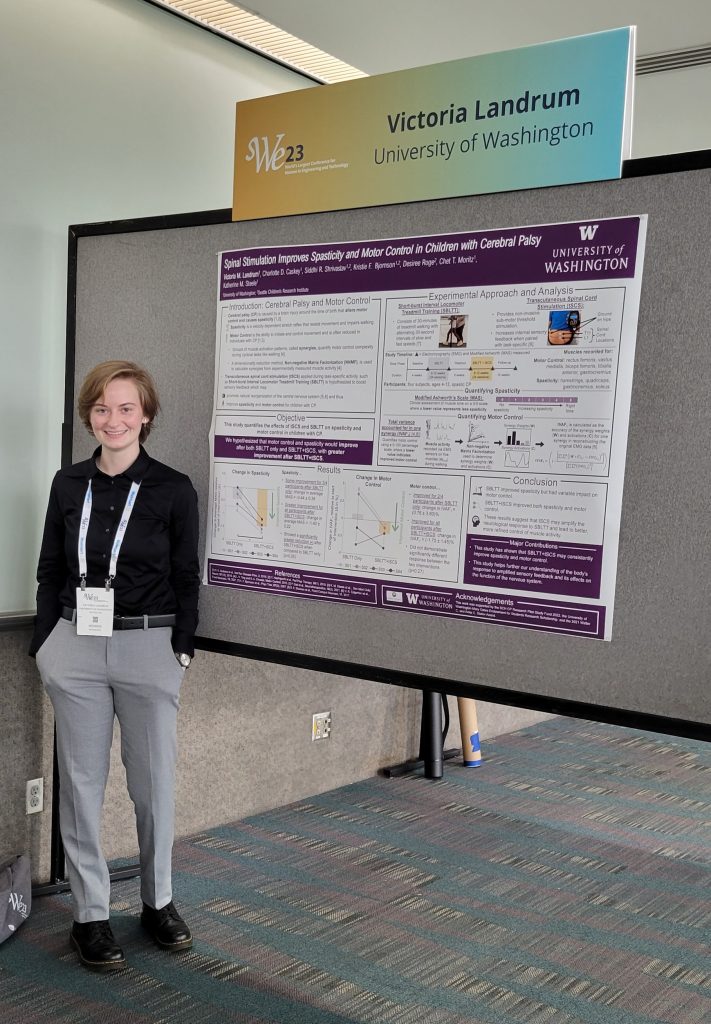
Tori placed 3rd in the undergraduate student division for her poster titled “Spinal Stimulation Improves Spasticity and Motor Control in Children with Cerebral Palsy”. Charlotte placed 1st in the graduate student division for her work titled “Machine Learning for Quantifying Rehabilitation Response in Children with Cerebral Palsy.
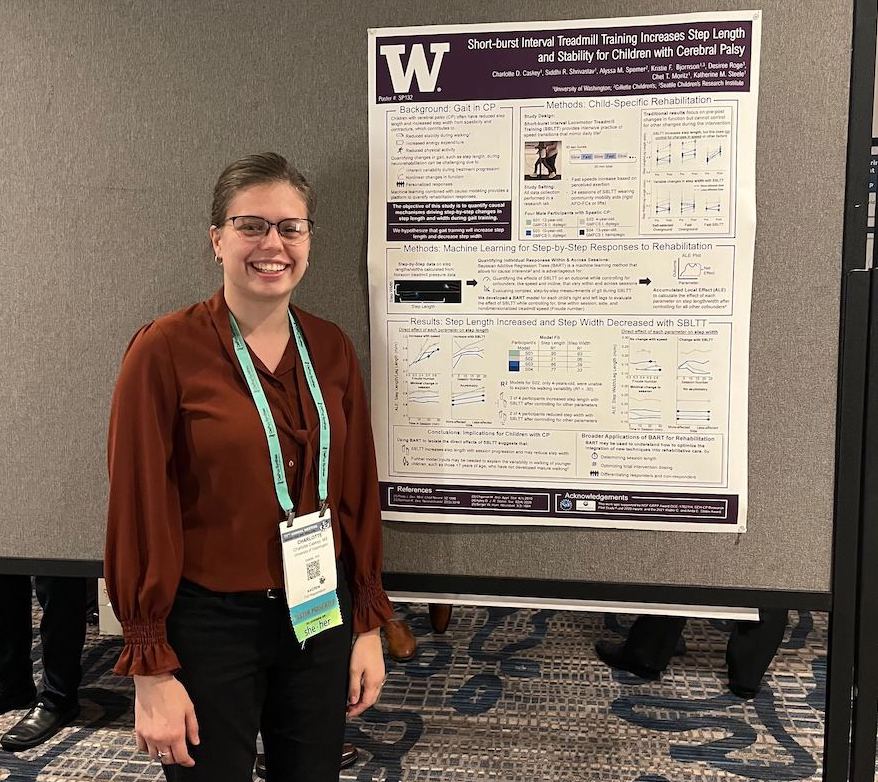
Lab members, Charlotte Caskey andMia Hoffman attended the 2023 American Academy for Cerebral Palsy and Developmental Medicine (AACPDM) Annual Meeting in Chicago, IL on September 10-13, 2023.
Charlotte gave a poster presentation on “Short-Burst Interval Treadmill Training Increases Step Length and Stability for Children with Cerebral Palsy.”
Mia gave a podium presentation during the Early Detection and Diagnosis session on “Quantifying the Activity Levels of Toddlers with Down Syndrome Playing in a Partial Body Weight Support System.“
Two lab members, Nicole Zaino and Mia Hoffman attended the annual Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) Conference on July 24-26 in New Orleans, LA.
Big congratulations to Mia Hoffman for being selected as an awardee in the Student Scientific Paper Competition (SSPC).
Journal Article in Journal of NeuroEngineering & Rehabilitation
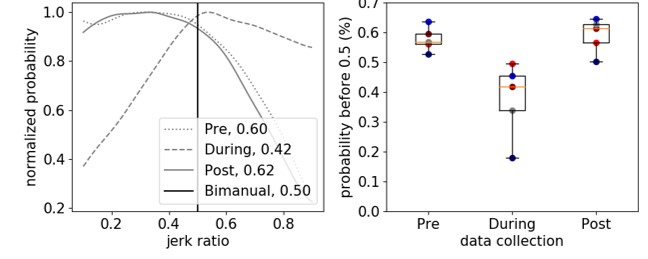
(Left) Example of jerk ratio distribution for one child with cerebral palsy before, during, and after constraint induced movement therapy. (Right) Summary metric of jerk ratio (jerk ratio-50) for all five children with cerebral palsy.
Background
Accelerometers have become common for evaluating the efficacy of rehabilitation for patients with neurologic disorders. For example, metrics like use ratio (UR) and magnitude ratio (MR) have been shown to differentiate movement patterns of children with cerebral palsy (CP) compared to typically-developing (TD) peers. However, these metrics are calculated from “activity counts” – a measure based on proprietary algorithms that approximate movement duration and intensity from raw accelerometer data. Algorithms used to calculate activity counts vary between devices, limiting comparisons of clinical and research results. The goal of this research was to develop complementary metrics based on raw accelerometer data to analyze arm movement after neurologic injury.
Method
We calculated jerk, the derivative of acceleration, to evaluate arm movement from accelerometer data. To complement current measures, we calculated jerk ratio (JR) as the relative jerk magnitude of the dominant (non-paretic) and non-dominant (paretic) arms. We evaluated the JR distribution between arms and calculated the 50th percentile of the JR distribution (JR50). To evaluate these metrics, we analyzed bimanual accelerometry data for five children with hemiplegic CP who underwent Constraint-Induced Movement Therapy (CIMT) and five typically developing (TD) children. We compared JR between the CP and TD cohorts, and to activity count metrics.
Results
The JR50 differentiated between the CP and TD cohorts (CP = 0.578±0.041 before CIMT, TD = 0.506±0.026), demonstrating increased reliance on the non-dominant arm for the CP cohort. Jerk metrics also quantified changes in arm use during and after therapy (e.g., JR50 = 0.378±0.125 during CIMT, 0.591 ± 0.057 after CIMT). The JR was strongly correlated with UR and MR (r = -0.92, 0.89) for the CP cohort. For the TD cohort, JR50 was repeatable across three data collection periods with an average similarity of 0.945±0.015.
Conclusions
Acceleration-derived jerk captured differences in motion between TD and CP cohorts and correlated with activity count metrics. The code for calculating and plotting JR is open-source and available for others to use and build upon. By identifying device-independent metrics that can quantify arm movement in daily life, we hope to facilitate collaboration for rehabilitation research using wearable technologies.
Code
The algorithm for calculating jerk ratio, as well as user-friendly code to produce plots similar to the figure above are provided open-source as Python 3.6 code as a Python Jupyter Notebook within Google Colab. With this resource, research groups can use existing or newly created data from accelerometers to analyze jerk ratio as a complementary metric to existing measures, enabling comparison between research studies or centers that may rely on different sensors and activity count algorithms.
In collaboration with Gillette Children’s Hospital and University Hospital Pellenberg we examined whether associations between treatment outcomes and muscles synergies are robust between clinical centers.
Objective: To determine whether patient-specific differences in motor control quantified using muscle synergy analysis were associated with changes in gait after treatment of cerebral palsy (CP) across 2 clinical centers with different treatments and clinical protocols.
Design: Retrospective cohort study.
Setting: Clinical medical center.
Participants: Center 1: children with CP (n=473) and typically developing (TD) children (n=84). Center 2: children with CP (n=163) and TD children (n=12).
Interventions: Standard clinical care at each center.
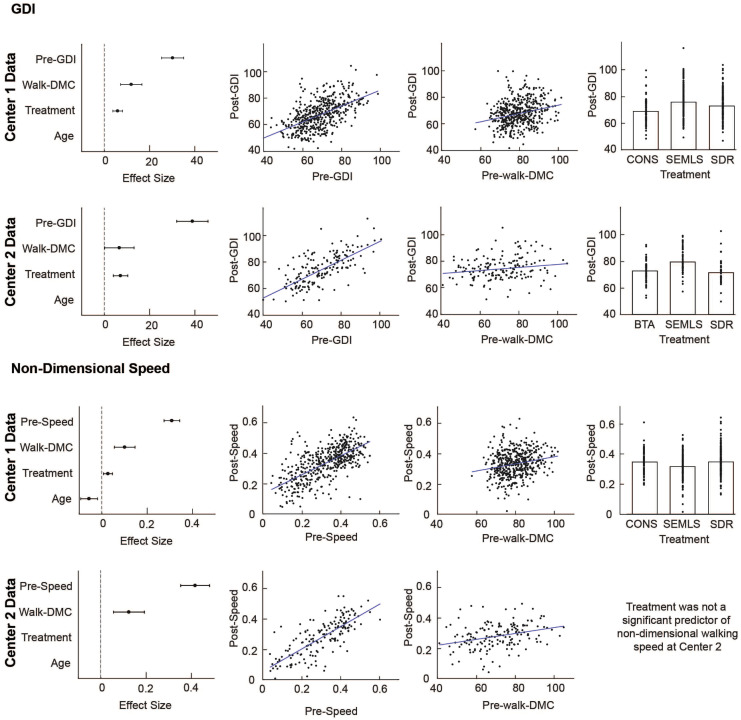
Main outcome measures: The Dynamic Motor Control Index During Walking (walk-DMC) was computed from electromyographic data during gait using muscle synergy analysis. Regression analysis was used to evaluate whether pretreatment walking speed or kinematics, muscle synergies, treatment group, prior treatment, or age were associated with posttreatment changes in gait at both clinical centers.
Results: Walk-DMC was significantly associated with changes in speed and kinematics after treatment with similar regression models at both centers. Children with less impaired motor control were more likely to have improvements in walking speed and gait kinematics after treatment, independent of treatment group.
Conclusions: Dynamic motor control evaluated with synergy analysis was associated with changes in gait after treatment at both centers, despite differences in treatments and clinical protocols. This study further supports the finding that walk-DMC provides additional information, not captured in traditional gait analysis, that may be useful for treatment planning.